Rumbidzayi Zinyuke
Senior Health Reporter
WHEN she discovered she was pregnant, 17-year-old Rudo (full name withheld) felt her world collapse.
“The first emotion that engulfed me was disappointment. I felt like I had let down my family. Fear quickly followed. I was afraid of my parents, my siblings and even my church community,” she said.
Overwhelmed by shame, she withdrew into silence, choosing isolation over seeking help.
In her confusion, she convinced herself she had to handle the situation alone, without fully understanding the risks or consequences.
In desperation, she turned to unsafe methods.
“I went and bought a large packet of pills and took all of them at once. In that moment, I did not value my life; I was more concerned about what people would think of me. It felt like it was the only way out,” she said.
Within hours, she was bleeding heavily and was rushed to hospital — becoming one of many young Zimbabwean girls who end up in emergency wards after unsafe abortion attempts.
Her ordeal did not end at the hospital.
“Abortion regret is real. It is complex, deeply personal and often carried in silence,” she said.
“I faced long-term emotional pain, constant ‘what if’ thoughts and a deep internal struggle that I am still dealing with today.”
Rudo’s story is not isolated.
It reflects the lived reality of thousands of women and girls across Zimbabwe navigating unintended pregnancies within a system shaped by restrictive laws, social stigma and limited access to services.
Zimbabwe’s abortion laws are governed by the Termination of Pregnancy Act of 1977, which permits abortion only under specific circumstances: when the life or physical health of the mother is at risk, in cases of rape or incest or where there is severe foetal abnormality.
Even in these instances, the process is tightly regulated, often requiring approval from multiple medical practitioners and, in some cases, the courts.
On paper, the law is clear, but in practice the situation is far more complex.
Globally, about six in every 10 unintended pregnancies end in termination, driven by factors such as limited access to contraception, contraceptive failure and financial hardship.
Zimbabwe mirrors many of these realities.
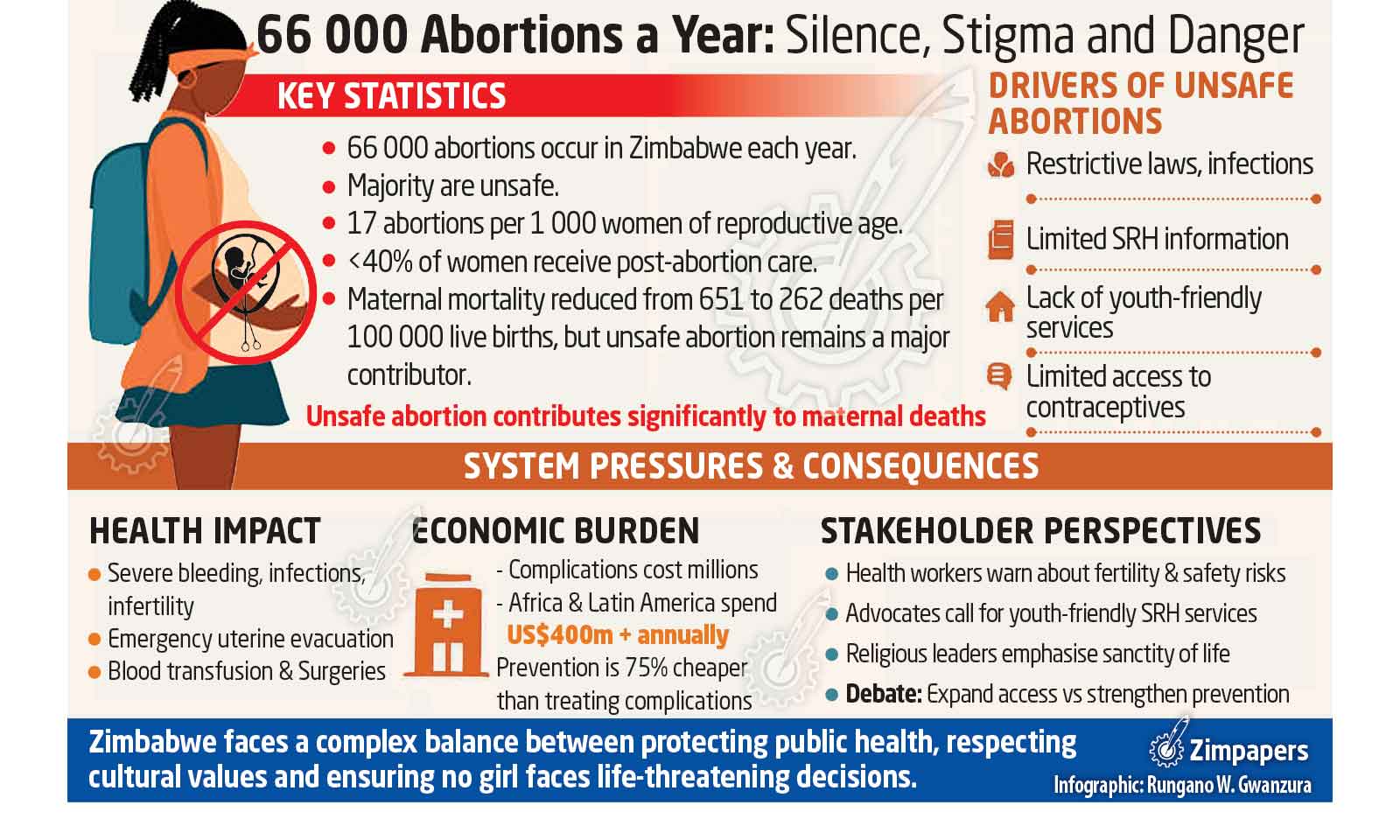
While the country has made notable progress in reducing maternal mortality — from 651 deaths per 100 000 live births to 262 — unsafe abortion remains a significant contributor to maternal deaths.
According to the World Health Organisation (WHO), studies estimate that 66 000 induced abortions occur in Zimbabwe each year, the majority of them unsafe.
This translates to 17 abortions per 1 000 women of reproductive age.
Of these, fewer than 40 percent receive post-abortion care in health facilities.
Behind these figures are hospital wards that continue to receive women with severe bleeding, infections and other complications — a daily reality for health workers.
What this means is that women do not stop seeking abortions because the process is restricted.
Instead, many are pushed outside the formal health system into unsafe environments, informal networks and silence.
Gaps in access and information
For many, the issue extends beyond legality to deeper structural gaps in access to services and information.
From a clinical perspective, health practitioners say the problem is tied to broader healthcare system challenges.
Dr David Broom, a health practitioner and sexual and reproductive health advocate, said discussions around abortion must consider medical realities and system capacity.
“There are no purely safe options. No medical procedure is without risk. It is important for people to understand the possible consequences, including risks to future fertility,” he said.
“That girl may never conceive again and the risk of death is very real.”
Dr Broom noted that the healthcare system is not adequately equipped to deal with this scourge.
Executive director of the Community Working Group on Health Mr Itai Rusike said weaknesses in the health system continued to leave vulnerable groups exposed.
He pointed out that while reproductive health rights are provided for in the Constitution, access to services remains uneven across communities.
“Working within communities, we find very limited places or information centres for accessing sexual and reproductive health, including health facilities,” said Mr Rusike.
“This information should be available across the life course, but we see many areas of neglect — especially for males, the young and the elderly. Women of childbearing age are catered for by maternal and child health (MCH) services.”
Mr Rusike stressed that adolescents, in particular, remained among the most underserved groups.
He said the absence of integrated, youth-friendly services created significant gaps, especially when young people faced unintended pregnancies and have nowhere to turn for guidance.
“There is a great need to educate communities on SRHR (sexual and reproductive health and rights) and ensure they are aware of the constitutional and legal provisions on sexual abuse of minors, safe abortion and other key components of SRHR,” said Mr Rusike.
“It is also important to provide information on complications and the availability — or lack — of services, so communities understand the magnitude of the problem and the consequences of inaction.”
Mr Rusike noted that these challenges were compounded by social and economic inequalities.
In some communities, the marginalisation of women and children increases their vulnerability to sexual abuse and exploitation, while also limiting their ability to seek or afford safe, legal services.
Consequences of silence
The absence of youth-friendly services, combined with stigma, continues to shape how women respond to unintended pregnancies.
Fear of judgement — from families, communities and sometimes even healthcare providers — discourages many from seeking help early.
As a result, many resort to unsafe methods.
Public health institutions have had to adapt to this reality.
Over the years, the Government, with support from partners, has strengthened post-abortion care services in public hospitals.
Women presenting with complications are treated regardless of the circumstances surrounding the abortion.
These services include emergency uterine evacuation, provision of antibiotics, blood transfusions and counselling.
While lifesaving, they also add pressure to already stretched health facilities.
Beyond physical complications, there is growing recognition of the psychological toll. Many women experience anxiety, depression and lingering emotional distress — often without access to mental health support.
Health system pressures and economic cost
Unsafe abortions are not only a public health concern, but also a burden on the healthcare system.
Economist Mr Titus Mukove explained that treating complications from unsafe abortions comes at a significant cost to both public and private institutions.
“There is a substantial financial burden when it comes to treating complications from unsafe abortions,” he said.
“These costs include hospital stays, blood transfusions and surgical procedures, which are all expensive and strain our public health system.”
He noted that the burden is not unique to Zimbabwe.
Across Africa and Latin America, the cost of managing complications runs into hundreds of millions of dollars annually, with Africa accounting for a significant
share.
“Studies across Africa and Latin America estimate that the cost exceeds US$400 million annually, with Africa alone accounting for over US$150 million,” said Mr Mukove.
“Zimbabwe is part of this broader picture, where limited resources are already under pressure.”
Mr Mukove said prevention could significantly reduce both health and economic costs.
“Providing contraceptive services and preventive sexual and reproductive health care is far less costly than managing emergency complications,” he said.
“In some studies, prevention has been shown to cost as little as a quarter of what is spent on treating complications.”
Debating reform and responsibility
Zimbabwe is engaged in broader discussions around sexual and reproductive health policies, including a review of the Medical Services Amendment Bill.
Earlier drafts of the Bill included Clause 11, a provision that sought to widen access to termination of pregnancy under specific conditions. However, this clause was later removed.
Advocacy groups under the Sexual and Reproductive Health Best Interest of the Child movement welcomed the decision, arguing that such changes required deeper national dialogue.
At the centre of the debate lies a fundamental question: Should policy prioritise expanding access to abortion services or should it focus more on prevention, family support systems and protection mechanisms?
Stakeholders remain divided, reflecting the complexity of the issue.
For religious leaders, the discussion extends beyond policy into values and societal direction.
Bishop Never Muparutsa, president of the Evangelical Fellowship of Zimbabwe, said framing abortion as part of reproductive health was problematic.
“The question is how abortion impacts communities and erodes the sanctity of life,” he said.
“Lumping abortion together with reproductive health services is a fundamental error, because the two are not the same and should be treated separately.”
Bishop Muparutsa cautioned against expanding access, arguing that it could have long-term social and psychological consequences.
Instead, he called for a stronger focus on prevention, community support and helping young women carry pregnancies safely.
“Our current legal provisions are more than sufficient. I believe it is not so much a stigma issue, but an issue of increased provisions of positive, lifesaving (not life-taking) services,” he said.
“The provision of community forums where the young and the old share life and challenges will assist in addressing stigma that produces shame and rejection for unintended pregnancies.
“Such forums will also help shape good values that respect life and emphasise ubuntu/unhu, where there is care and full concern for each other in all circumstances of life.”
Bishop Muparutsa highlighted broader social drivers such as poverty, peer pressure and family breakdown, stressing the need for holistic interventions that address the root causes of unintended pregnancies.
A complex national question
As the debate continues, abortion in Zimbabwe remains a deeply layered issue, intersecting public health, law, economics, culture and personal experience.
On one hand, there is clear evidence of the health risks associated with unsafe abortions, their contribution to maternal deaths and the strain they place on the healthcare system.
On the other hand, there are strong calls to uphold cultural and moral values, strengthen family structures and prioritise prevention.
Between these positions are the lived realities of women and girls like Rudo, who often face these decisions in isolation, without adequate information or support. For her, the experience remains a defining moment.
“If I had known the options available to me and if I had understood that I was not alone, I believe I would have made a different choice. I needed guidance, not fear,” she said.
Her story underscores that beyond laws and policies, access to accurate information, supportive communities and responsive health systems can shape outcomes in profound ways.
As Zimbabwe continues to reflect on its laws and policies, the challenge will be to strike a careful balance — one that addresses public health realities, respects societal values and ensures that no woman or girl is left to navigate such life-altering decisions alone.