
Rumbidzayi Zinyuke
Health Buzz
On some mornings, 29-year-old Rudo (not her real name) wakes up feeling as though her body has betrayed her.
Her joints ache as if she has run a marathon, her skin burns after only a short walk in the sun, and her energy drains so quickly that simple tasks like cooking, doing the dishes and even socialising feel impossible.
On better days, she looks perfectly healthy, which confuses even her closest family and friends.
But beneath the surface, Rudo is fighting lupus, a chronic autoimmune disease that does not just attack her body but also reshapes her everyday life in unpredictable ways.
A disease that fights from within
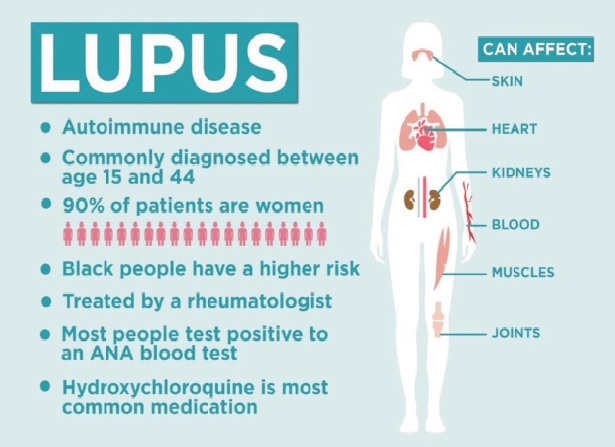
Lupus (systemic lupus erythematosus) is a condition in which the immune system, the very system meant to protect us, turns against the body’s own tissues. The result is widespread inflammation that can affect virtually any organ: skin, joints, kidneys, heart, lungs, blood and even the brain.
Doctors sometimes call it the great imitator because its early symptoms resemble those of many other illnesses, leading to frequent delays in diagnosis.
The World Health Organisation (WHO) estimates that about 3,4 million people worldwide are affected, with women accounting for nearly 90 percent of cases, especially those of childbearing age.
In Zimbabwe and across Africa, lupus is not as rare as once thought. Studies dating back more than two decades identified renal complications as a common and dangerous outcome of the disease.
More recent hospital-based studies across sub-Saharan Africa confirm that lupus is one of the most common inflammatory rheumatic conditions seen by clinicians, yet often under-recognised.
The gender bias of lupus is striking.
In Africa, studies have found up to 100 percent of patients in certain cohorts to be women. The disease tends to strike in the prime of life, often between the ages of 15 and 45, when women are pursuing education, starting families or advancing in careers.
This means the ripple effects extend far beyond the patient. Families lose caregivers, workplaces lose productivity, and communities lose the contributions of young women who might otherwise be in their most productive years.
For Zimbabwean women, the burden is compounded by the structure of livelihoods. Many women depend on outdoor activities such as farming or trading in open markets. Yet exposure to the sun is one of the strongest triggers for lupus flares, putting their health directly at odds with economic survival.
The symptoms of lupus can be wide-ranging and elusive.
For many patients, fatigue is the first and most persistent sign, a crushing exhaustion that does not improve with rest. Others experience joint pain, swelling, or skin rashes, including the characteristic butterfly-shaped rash across the cheeks.
But these early signs are easily confused with more common illnesses such as malaria, arthritis or skin allergies. Some patients are only diagnosed after severe complications like kidney inflammation, chest pain or seizures emerge.
In a healthcare system where resources are already stretched, the absence of widespread testing for lupus antibodies means that diagnosis often takes months or even years. For many, by the time the disease is identified, organs have already been damaged.
Despite its challenges, lupus is treatable. Drugs such as hydroxychloroquine, steroids, and immunosuppressants can control inflammation and reduce flares. Lifestyle modifications loke avoiding direct sun, balancing rest and exercise, and careful pregnancy planning, have been shown to improve outcomes.
But access remains uneven. In Zimbabwe, essential medicines for lupus are not always available in public facilities, forcing patients to rely on expensive private pharmacies. Dialysis and kidney biopsies, critical for those with lupus nephritis, are out of reach for many. The shortage of specialist doctors also further complicates care.
Globally, biologic drugs are offering hope for patients with resistant disease. But their high cost and intensive monitoring requirements keep them far from reach for most African patients.
Living with lupus is not only about managing physical symptoms. The unpredictability of the disease brings mental and emotional tolls. Frequent flares, “brain fog,” and fatigue interfere with education and work, while social withdrawal and misunderstanding from peers deepen isolation.
Depression and anxiety are common but rarely addressed in routine care. In Zimbabwe, where mental health services are scarce and often stigmatised, patients like Rudo face a double burden: fighting a misunderstood illness while also navigating emotional distress with little formal support.
Perhaps the greatest challenge for Zimbabwe and the wider region is the lack of data. Unlike diseases such as HIV, malaria, or tuberculosis, lupus does not feature in national health statistics. Without reliable numbers, policymakers struggle to budget for medicine procurement, invest in diagnostic equipment, or train specialists.
This invisibility also means lupus remains outside major health campaigns and awareness programmes. While communities are educated on hypertension, diabetes, or HIV prevention, autoimmune diseases are hardly mentioned. Yet the reality is that lupus is quietly reshaping lives and straining households in ways that remain undocumented.
Zimbabwe’s National Development Strategy 1 (NDS1) and Vision 2030 set out clear goals to ensure universal health coverage and equitable access to care. If these aspirations are to be realised, conditions like lupus—though less common than infectious diseases—cannot be ignored.
Expanding early diagnostic capacity, ensuring steady supplies of essential medicines and integrating mental health and patient education into chronic care frameworks would align directly with the goal of “leaving no one and no place behind.”
Partnerships with civil society and patient advocacy groups could also raise awareness and reduce stigma.
Lupus thrives in delay and invisibility. But evidence from countries that have prioritised early detection shows that outcomes can improve dramatically when patients are diagnosed early and treated consistently.
For Zimbabwe, the path forward lies in educating communities and frontline health workers to recognise warning signs. It is also important to secure affordable supplies of essential medicines and diagnostics.
Embedding psychosocial care into chronic disease programmes and establishing registries and local studies to track prevalence, treatment outcomes, and patient needs is also key.
For Rudo and thousands of women like her, lupus is not an abstract medical condition but a daily battle. It shapes when they work, how they interact, whether they can safely start a family, and how long they may live.
The disease may remain invisible to the casual eye, but its burden is very real. With greater awareness, stronger health system support, and recognition within Zimbabwe’s national health priorities, lupus can be transformed from a silent, neglected illness into a manageable condition.
The challenge is clear: lupus must not remain hidden in the shadows.
Feedback: [email protected]

