
Rumbidzayi Zinyuke-Health Buzz
IN a corner of a small rural clinic, a woman sits quietly as she waits for someone to call her name.
She had walked in for what she thought was a routine check-up, a nagging discomfort she had brushed aside for more than a year while focusing on work, children and errands that seemed somehow more urgent.
When the doctor raised the possibility of cervical cancer, her eyes widened in fear.
For her, the word “cancer” felt heavy, distant and unreal, as though it belonged to strangers on television and not to ordinary women like her.
Yet this experience mirrors the reality of thousands of Zimbabwean women who silently confront symptoms they barely understand.
Cervical cancer is not a faraway problem. It is in our neighbourhoods, workplaces and homes. It affects women who often put family ahead of their own health, women who may never have heard of HPV, women who assume they are safe because they feel no pain.
This is one of the most preventable cancers, yet it remains one of the deadliest for African women.
Cervical cancer develops in the cells of the cervix, usually after years of persistent infection with high-risk types of the human papillomavirus (HPV), a virus transmitted primarily through sexual contact.
Although most sexually active people encounter HPV at some point, in many women the infection clears naturally. In others, however, it lingers and gradually causes changes that can develop into cancer over 10 to 15 years.
What makes cervical cancer particularly dangerous is that it often produces no symptoms in the early stages. When signs eventually appear, unusual vaginal bleeding, pelvic pain, pain during intercourse or an abnormal discharge, the disease is often already advanced, making treatment more complex and survival rates lower.
Yet, unlike many other cancers, cervical cancer is almost entirely preventable. HPV vaccination before exposure to the virus significantly reduces the likelihood of infection with high-risk strains.
The World Health Organisation advocates vaccinating girls aged nine to fourteen, and Zimbabwe has been among the more successful African countries in rolling out the HPV vaccine.
Since introducing it into the national immunisation schedule in 2018, the country has achieved high coverage, reaching about 89 percent of targeted girls. This success is largely due to school-based vaccination campaigns and community mobilisation, though challenges persist for girls who are out of school, those in remote areas, or families who are hesitant due to myths and misinformation about vaccines.
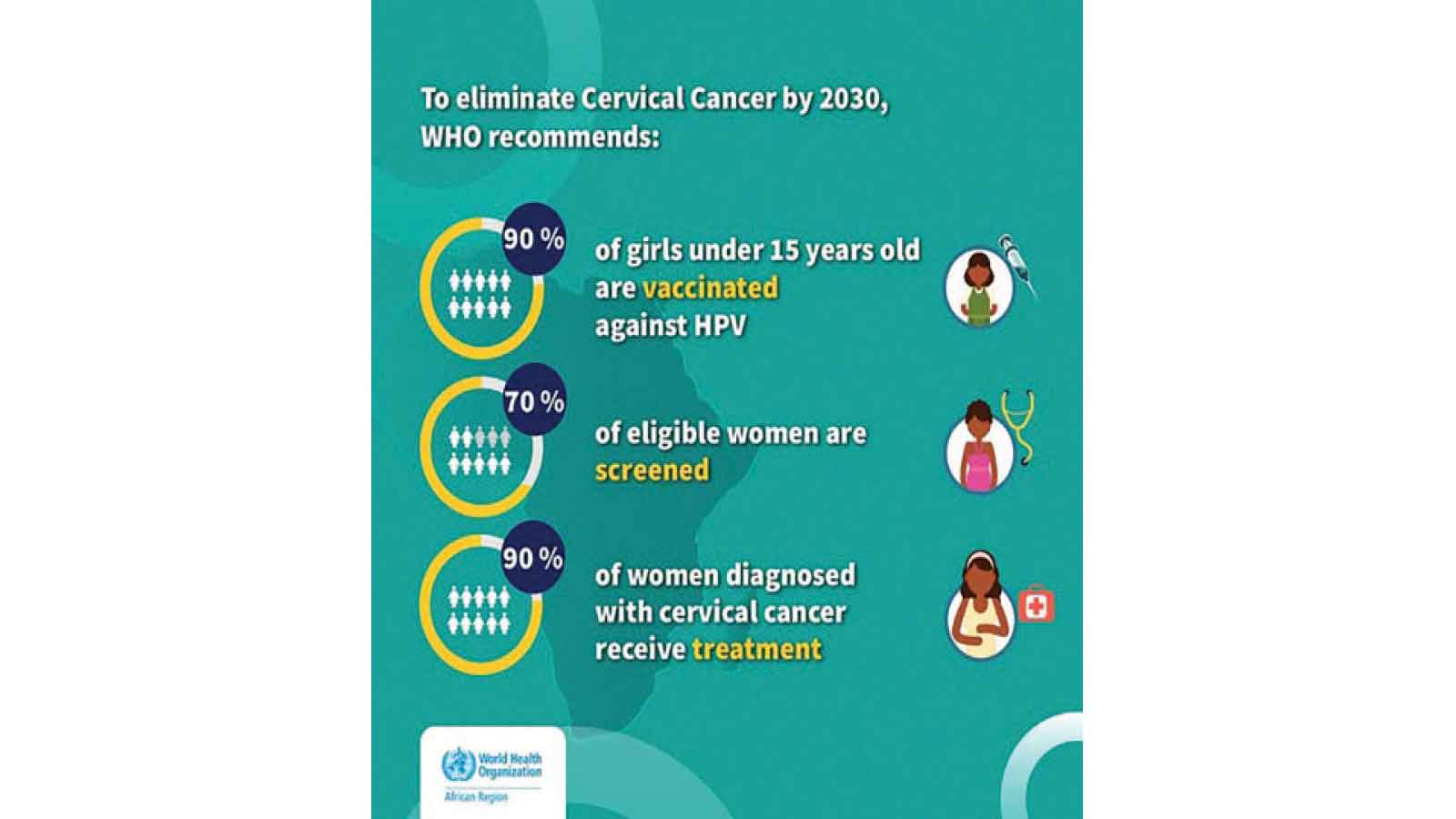
Zimbabwe aims to meet WHO’s 90-70-90 targets (90 percent vaccinated, 70 percent screened, 90 percent treated) to eliminate cervical cancer as a public health problem by 2030.
Screening is the second critical pillar of preventing cervical cancer, because it detects abnormalities long before they turn into cancer.
Screening methods such as Visual Inspection with Acetic Acid (VIAC) and HPV DNA testing are now available in Zimbabwe.
Health experts recommend that women between the ages of 30 and 49 undergo regular screening. But despite the availability of services, screening rates remain low.
Only one in five eligible Zimbabwean women has ever been screened. Rural women face even greater challenges like limited facilities, transport costs and long distances to clinics which often deter them from seeking care.
Beyond these logistical hurdles, myths and cultural beliefs also suppress uptake. Some women believe screening is painful, humiliating or unnecessary if they have no symptoms. Others simply do not know that cervical cancer starts long before symptoms appear.
A study published in 2021 showed that only 24 percent of Zimbabwean women of reproductive age accurately linked HPV to cervical cancer, revealing significant gaps in public understanding.
Cervical cancer is a major crisis in Africa, with 19 of the 20 countries with the highest burdens located on the continent, and Zimbabwe is among the worst hit, ranking high globally for incidence, with about 3 500 new cases annually and high mortality.
The burden of cervical cancer is worsened by systemic and structural barriers. Many rural clinics lack the equipment or trained staff needed to conduct screening or provide follow-up care. Health workers are often overstretched, and women may not receive the counselling or support necessary to navigate next steps after a positive screening.
Treatment services are frequently centralised, with radiotherapy machines in urban hospitals sometimes breaking down or operating below capacity. This means that many women diagnosed with cervical cancer have to travel long distances for treatment or face long waiting periods, both of which can contribute to late initiation of care.
Costs also remain a major barrier. Although some services are subsidised, diagnostic tests, specialised treatment and palliative care often fall beyond what many families can afford.
Against this background, awareness becomes more than a simple public health slogan, it becomes a lifeline.
January, recognised globally as Cervical Cancer Awareness Month, offers Zimbabwe an opportunity to turn attention toward this preventable disease. It is a moment to amplify education campaigns, encourage women to get screened, and remind families, communities and policymakers that cervical cancer can be eliminated with sustained effort.
Using this month strategically, through media messaging, community outreach and strengthening health services, can significantly improve awareness and empower more women to protect themselves throughout the year.
When women understand how cervical cancer develops, how it can be prevented, why screening matters and where to access services, they are more likely to take steps that protect their health.
Awareness dispels myths, challenges stigma and empowers communities. It also encourages men to support the women in their lives by advocating for vaccination, encouraging partners to get screened and understanding the disease as a shared family concern rather than a women’s issue alone.
There is much Zimbabwe can do to strengthen cervical cancer prevention and control.
First, community-centred education campaigns must intensify, especially in rural and peri-urban areas where misinformation is rife. Community health workers, who are often trusted voices, should be empowered with the training and resources needed to educate households and mobilise screening.
Second, screening services need to be decentralised. Mobile clinics, self-sampling HPV kits and integrated outreach services can bridge the gap for women who cannot reach health facilities.
Third, the HPV vaccination programme must be sustained and expanded so that every eligible girl, whether in school or out of school, has access. Continuous engagement with parents, religious leaders and educators is essential to maintain confidence in the vaccine.
Finally, investment in treatment infrastructure is crucial. Reliable radiotherapy machines, accessible chemotherapy and well-supported palliative care can drastically improve outcomes for women diagnosed with cervical cancer.
The truth is, cervical cancer should no longer be claiming the lives of Zimbabwean women.
Not when prevention tools exist. Not when early detection saves lives. Not when awareness can transform fear into action.
Awareness opens the door to prevention, to timely care and to hope. The more we talk about cervical cancer openly, accurately and compassionately, the more lives we can save.
It is time to make cervical cancer screening, HPV vaccination and women’s health conversations an everyday part of community life.
Because early knowledge leads to early action, and early action saves lives.
Feedback: [email protected]

