Rumbidzayi Zinyuke
Health Buzz
It is common in many communities to assign labels to people living with mental health problems. Often, they are simply called “mapenzi” a word loosely used to describe someone as “crazy” or “insane.” The explanation rarely goes beyond the label.
For many, the cause is quickly attributed to witchcraft (akaroiwa) or personal wrongdoing (pane zvaakaita), with blame directed at the individual rather than showing concern for possible illness.
Rarely do we pause to consider that some of these experiences may be symptoms of a medical condition.
Mental illnesses, to be precise.
When conversations about mental health do happen, schizophrenia is often among the most misunderstood conditions. Popular culture and public imagination have reduced it to images of unpredictability, violence, or the inaccurate idea of “split personalities,” creating fear instead of understanding.
Yet schizophrenia is not a character flaw, punishment, or supernatural phenomenon. It is a serious mental health condition that affects how a person perceives reality, thinks, feels, behaves, and connects with the world around them.
For millions of people globally, schizophrenia is not simply a diagnosis recorded in a medical file. It can influence education, employment, family relationships, social participation, and overall quality of life.
According to the World Health Organisation (WHO), schizophrenia affects approximately 23 million people worldwide, about 1 in every 345 people globally and around 1 in every 233 adults.
While it is less common than many other mental disorders, its effects can be life-altering because symptoms may interfere with nearly every aspect of daily functioning.
Schizophrenia most commonly develops during late adolescence and early adulthood, a stage already defined by major decisions around education, work, relationships, and identity. Symptoms also tend to appear earlier among men than women, although the condition affects people across all genders and social groups.
Understanding schizophrenia begins with understanding what happens during the illness.
The condition is characterised by psychosis, a significant change in the way reality is experienced and interpreted. This does not mean a person is imagining problems or deliberately choosing unusual beliefs. Rather, schizophrenia affects brain processes involved in interpreting thoughts, emotions, experiences, and information.
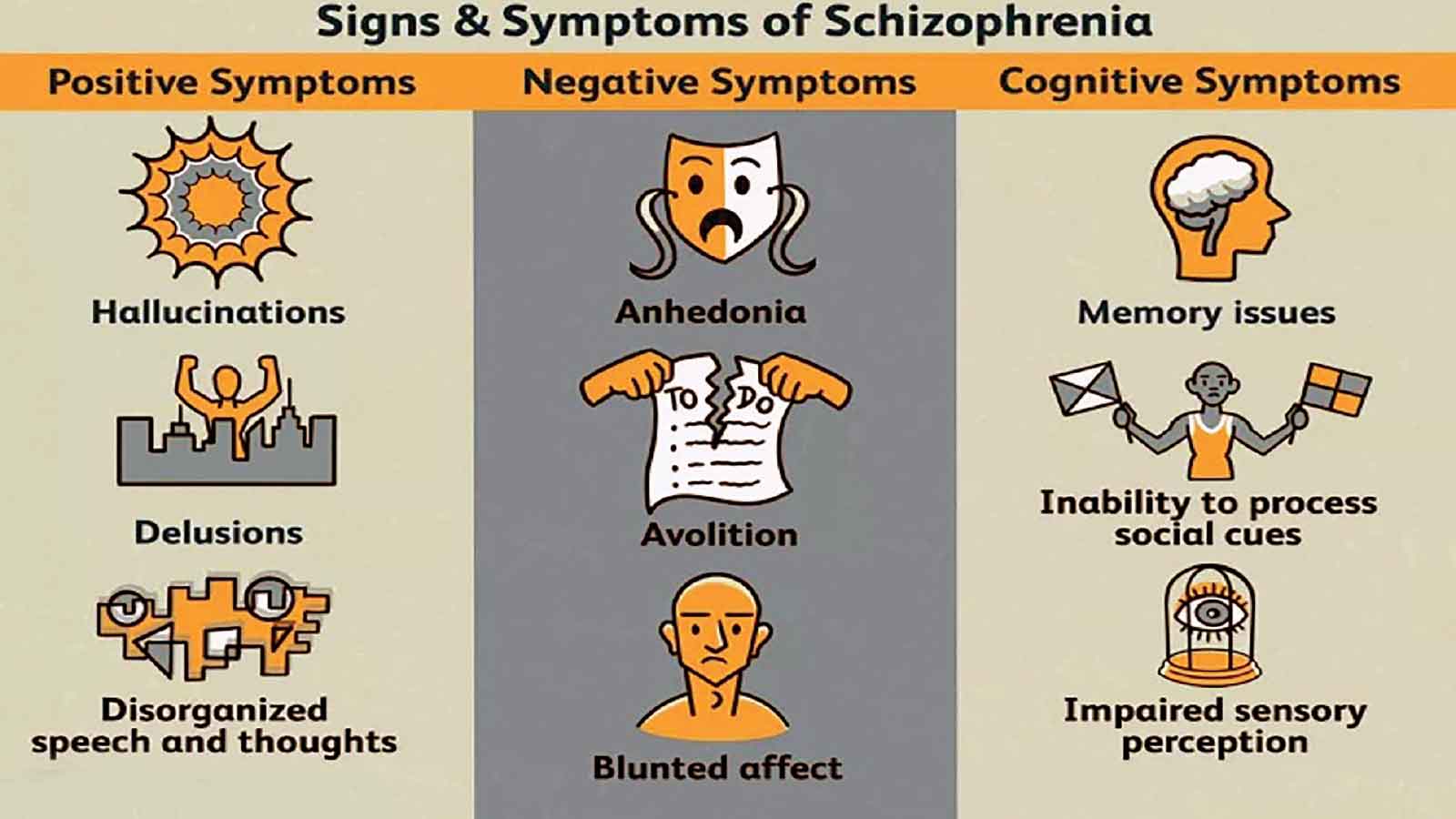
Symptoms may present in different ways. Some people experience persistent delusions, strong beliefs held despite evidence showing otherwise. Others experience hallucinations, where sensations such as hearing voices, seeing things, or feeling touch occur without an external source.
Thinking and communication may also become affected. Disorganised thinking can make speech appear disconnected, difficult to follow, or unrelated to the conversation. Behaviour may become disorganised or interfere with daily routines and social relationships.
Not all symptoms are obvious to others.
Negative symptoms, which are often overlooked, may involve reduced emotional expression, limited speech, social withdrawal, reduced motivation, and difficulty experiencing interest or pleasure in daily activities. To outsiders, someone may appear uninterested or emotionally absent when in reality they are dealing with symptoms of an illness.
Cognitive changes may also affect memory, attention, concentration, and problem-solving. These difficulties can make ordinary responsibilities, such as maintaining employment, attending school, managing finances, or sustaining relationships, more challenging.
Because schizophrenia affects so many areas of functioning, its impact extends far beyond the individual.
Families frequently become caregivers and supporters, often carrying emotional, financial, and social burdens without sufficient information or support. Fear and misunderstanding may delay help-seeking and deepen isolation.
Stigma remains one of the greatest obstacles to recovery.
Across communities, people living with schizophrenia may face rejection, discrimination, exclusion, and social judgement. Misconceptions linking the condition to violence continue to shape public attitudes despite evidence showing a more complex reality. Many people with schizophrenia are more vulnerable to victimisation and social disadvantage than posing danger to others.
WHO identifies stigma and discrimination as major contributors to poorer outcomes and reduced access to healthcare, education, housing, and employment opportunities.
The result is often a cycle: symptoms lead to exclusion, exclusion worsens distress, and distress delays treatment. There is also no single cause of schizophrenia.
Current evidence suggests the condition develops through an interaction between genetic vulnerability and environmental influences. Having a family history may increase risk but does not mean someone will automatically develop the illness.
Environmental factors associated with increased risk include complications during pregnancy or birth, exposure to severe stress, trauma, social adversity, and substance use. Heavy cannabis use has also been linked to elevated risk, particularly among individuals with other underlying vulnerabilities.
Experiences of chronic stress, isolation, and limited social support may influence when symptoms appear and how the condition progresses.
In Zimbabwe, comprehensive national data on schizophrenia remains limited, reflecting broader gaps in mental health reporting and investment. However, mental health professionals continue to identify psychotic disorders among major contributors to psychiatric admissions and long-term care needs.
The shortage of mental health specialists and limited community services mean many people may first present at local clinics or through family support systems before receiving specialised assessment.
Globally, the treatment gap remains significant.
WHO estimates that more than two out of every three people with psychosis do not receive specialist mental healthcare, while only about 29 percent access specialist services.
The challenge is therefore not simply diagnosis, it is access and quality of care.
For decades, institutional care became the dominant response to severe mental illness in many countries. However, WHO increasingly emphasises community-based approaches that integrate mental healthcare into general health systems and expand services closer to where people live.
Community care may include mental health centres, outreach programmes, supported housing, rehabilitation services, and integration into primary healthcare.
Recovery from schizophrenia is possible.
Recovery does not always mean the complete absence of symptoms or a return to life exactly as it was before illness. Rather, it means regaining stability, independence, confidence, and participation in daily life.
WHO notes that at least one in three people with schizophrenia can experience complete remission of symptoms.
Effective care often combines medication with psychological support, family education, therapy, and social rehabilitation. Supported employment and assisted living arrangements are also increasingly recognised as important parts of long-term recovery.
Families, communities, and health systems all play a role.
Education about schizophrenia can replace fear with understanding and reduce the isolation that so many affected individuals experience.
For Zimbabwe and many countries facing competing health priorities, schizophrenia offers a broader lesson. That mental health cannot remain separate from general healthcare.
Early recognition, accessible treatment, trained health workers, supportive families, and communities willing to challenge stigma can change outcomes.
Schizophrenia remains a serious condition, but it is not a hopeless one. With support, treatment, and social inclusion, many people living with schizophrenia can rebuild stability, participate meaningfully in society, and live with dignity.
The conversation begins not with fear, but with knowledge.
Feedback: [email protected]