Rumbidzayi Zinyuke
Health Buzz
Imagine living with a condition so uncommon that even experienced health professionals struggle to recognise it. Imagine moving from clinic to clinic, repeating the same story, watching symptoms worsen while answers remain elusive.
For millions of people around the world, this is not an exaggeration but everyday life.
Rare diseases, despite their name, are not rare in their collective impact. They affect hundreds of millions globally, yet in low to middle income countries like Zimbabwe, they remain largely invisible, misunderstood and under-prioritised in mainstream health conversations.
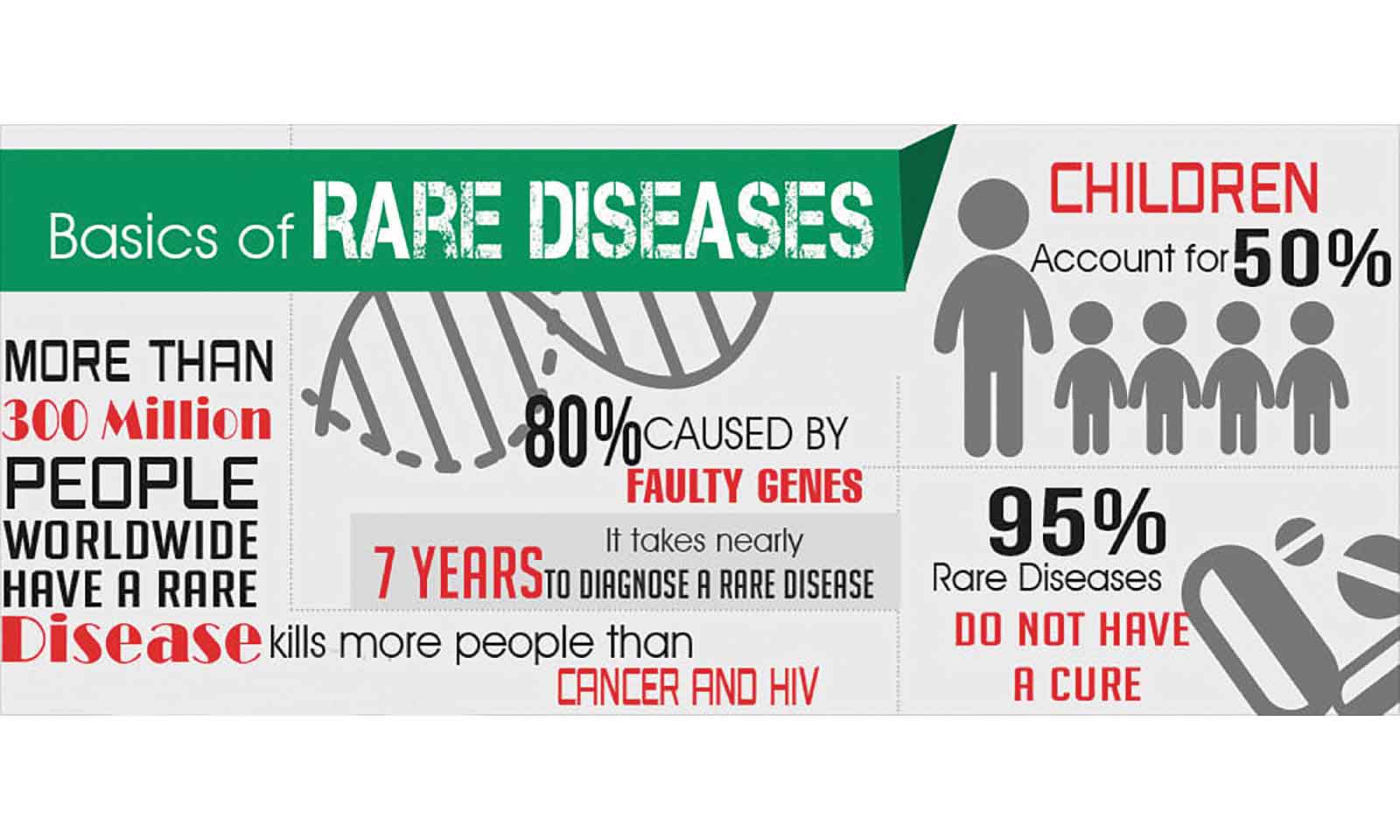
A rare disease is generally defined as one that affects fewer than one in 2 000 people. However, this definition can be misleading. There are more than 7 000 identified rare diseases worldwide, and when considered together, they affect an estimated 350 to 400 million people globally. That means roughly one in 10 people will live with a rare disease at some point in their lives.
Far from being isolated medical curiosities, rare diseases represent a significant but often hidden public health burden.
A striking feature of rare diseases is that most of them are genetic in origin. Experts estimate that about 70 percent manifest during childhood. Tragically, many of these conditions are severe, chronic and progressive.
Globally, about three in 10 children with a rare disease do not live to see their fifth birthday. Despite advances in medicine, more than 90 percent of rare diseases still have no approved treatment. For families, the diagnosis can feel like a life sentence delivered without a roadmap.
In Zimbabwe, the true scale of rare diseases remains unclear, largely because the country does not yet have a comprehensive national rare disease registry. Without systematic data collection, policymakers and health planners are left to rely on fragmented information from hospitals, advocacy groups and individual cases.
This lack of data makes it difficult to allocate resources, train specialists or ensure the availability of essential diagnostic tools. As a result, many patients endure what is often referred to globally as a “diagnostic odyssey”, years of consultations, misdiagnoses and inappropriate treatments before a correct diagnosis is finally made.
Among the rare conditions documented globally are disorders such as Wolfram syndrome, a genetic disease that can cause childhood-onset diabetes, vision loss and hearing impairment. Its prevalence ranges from about one in 160 000 to one in 770 000 people, depending on the population studied.
Another example is Hermansky–Pudlak syndrome, an inherited condition characterised by albinism, bleeding disorders and in some cases lung disease. It is estimated to affect around one in 500 000 people worldwide.
There are also congenital conditions such as imperforate anus, which occurs in approximately one in 5 000 live births and requires early surgical intervention.
Other conditions include Amyotrophic Lateral Sclerosis , a progressive neurodegenerative disease affecting voluntary muscle control, Ehlers-Danlos Syndrome, a connective tissue disorder leading to joint instability, chronic pain, and frequent injuries, Fabry Disease, a metabolic disorder causing nerve pain, gastrointestinal issues, and organ damage, treatable with enzyme therapy, Wilson’s Disease, a genetic condition causing copper accumulation in the liver and brain, leading to neurological and psychiatric symptoms.
While each of these conditions affects a small number of individuals, their cumulative effect across communities is substantial.
The signs and symptoms of rare diseases vary widely, which makes awareness crucial. Experts say in children, early warning signs may include developmental delays, failure to thrive, persistent feeding difficulties or unusual physical features present at birth.
Some children may experience recurrent infections due to underlying immune deficiencies, while others may show unexplained seizures or progressive neurological decline. In adolescents and adults, rare diseases can present with chronic pain, unexplained organ dysfunction, sensory impairments or unusual laboratory results that do not fit common diagnostic patterns. Because many of these symptoms overlap with more common conditions, rare diseases are often not immediately suspected.
Risk factors for rare diseases are also diverse. A significant proportion are inherited, meaning that a family history of unexplained illnesses, early deaths or similar symptoms may increase suspicion.
Consanguineous marriages, where close relatives marry, can also increase the likelihood of certain recessive genetic disorders, although this practice is not widespread in Zimbabwe compared to some other regions.
Environmental factors can also play a role in rare conditions, including exposure to toxins during pregnancy, infections that affect foetal development, or complications during childbirth. In some cases, spontaneous genetic mutations occur without any prior family history, underscoring the unpredictable nature of many rare disorders.
Beyond the physical toll, rare diseases carry heavy psychological and social consequences. Families often struggle with stigma, particularly in communities where unexplained medical conditions may be attributed to supernatural causes or moral failings. Parents may blame themselves, and patients may withdraw from social activities due to visible symptoms or disability.
The financial burden can be devastating. Repeated consultations, specialised tests and in some cases imported medications or surgical procedures can drain family savings. In a health system where many services require out-of-pocket payments, the cost of pursuing a diagnosis alone can be prohibitive.
Globally, there have been significant efforts to improve recognition and management of rare diseases. In the United States and parts of Europe, “orphan drug” policies have incentivised pharmaceutical companies to develop treatments for rare conditions that would otherwise be commercially unattractive.
International collaborations such as the International Rare Diseases Research Consortium have sought to coordinate research and share data across borders. These efforts have led to breakthroughs in gene therapy and targeted treatments for some conditions that were once considered untreatable.
However, access to such advances remains highly unequal. In many low- and middle-income countries, genetic testing services are limited and often expensive. Specialist care in fields such as medical genetics, metabolic medicine and paediatric neurology is scarce. Without adequate laboratory infrastructure, even recognising a rare metabolic or immunological disorder can be difficult. This gap underscores the importance of integrating rare diseases into broader health system strengthening efforts rather than treating them as peripheral issues.
The absence of a national registry in Zimbabwe represents a missed opportunity to understand and address a silent burden. A registry would not only quantify the number of affected individuals but also help identify patterns, guide training programmes for healthcare workers and support advocacy for resource allocation. It would provide a foundation for partnerships with regional and global research networks, potentially opening doors to clinical trials and new therapies.
Understanding rare diseases is also critical from a human rights perspective. The global commitment to Universal Health Coverage and the Sustainable Development Goals emphasises leaving no one behind. This principle applies just as much to a child born with a rare metabolic disorder in a rural district as it does to someone with a more common illness in an urban centre. Equity in healthcare means recognising that rarity does not diminish the value of a life.
For Zimbabwe, raising awareness about rare diseases begins with conversation. It means equipping frontline health workers to recognise red flags and refer patients appropriately. It means educating communities so that families seek medical help early rather than hiding symptoms out of fear or shame. It also means supporting patient advocacy groups that give a voice to those who might otherwise remain unheard.
Rare diseases challenge health systems because they demand specialised knowledge, long-term care and often costly interventions. Yet they also offer an opportunity to build more responsive, compassionate and inclusive healthcare structures. When systems are strengthened to detect and manage rare conditions, they often become better at handling complex cases in general.
Ultimately, the term “rare” should not translate into neglect. Behind every statistic is a person, a child struggling to reach developmental milestones, a teenager coping with progressive vision loss, a parent searching tirelessly for answers.
By shining a light on rare diseases, Zimbabwe can move closer to a health system that recognises every patient, counts every case and values every life, no matter how uncommon the diagnosis may be.
Feedback: [email protected]