
Rumbidzayi Zinyuke
Senior Health Reporter
WHAT was expected to be a year of consolidation in Zimbabwe’s fight against HIV instead became a stress test of the health system, as sudden shifts in global funding forced authorities to adapt quickly to keep prevention and treatment services running.
The year 2025 began on a note of cautious optimism.
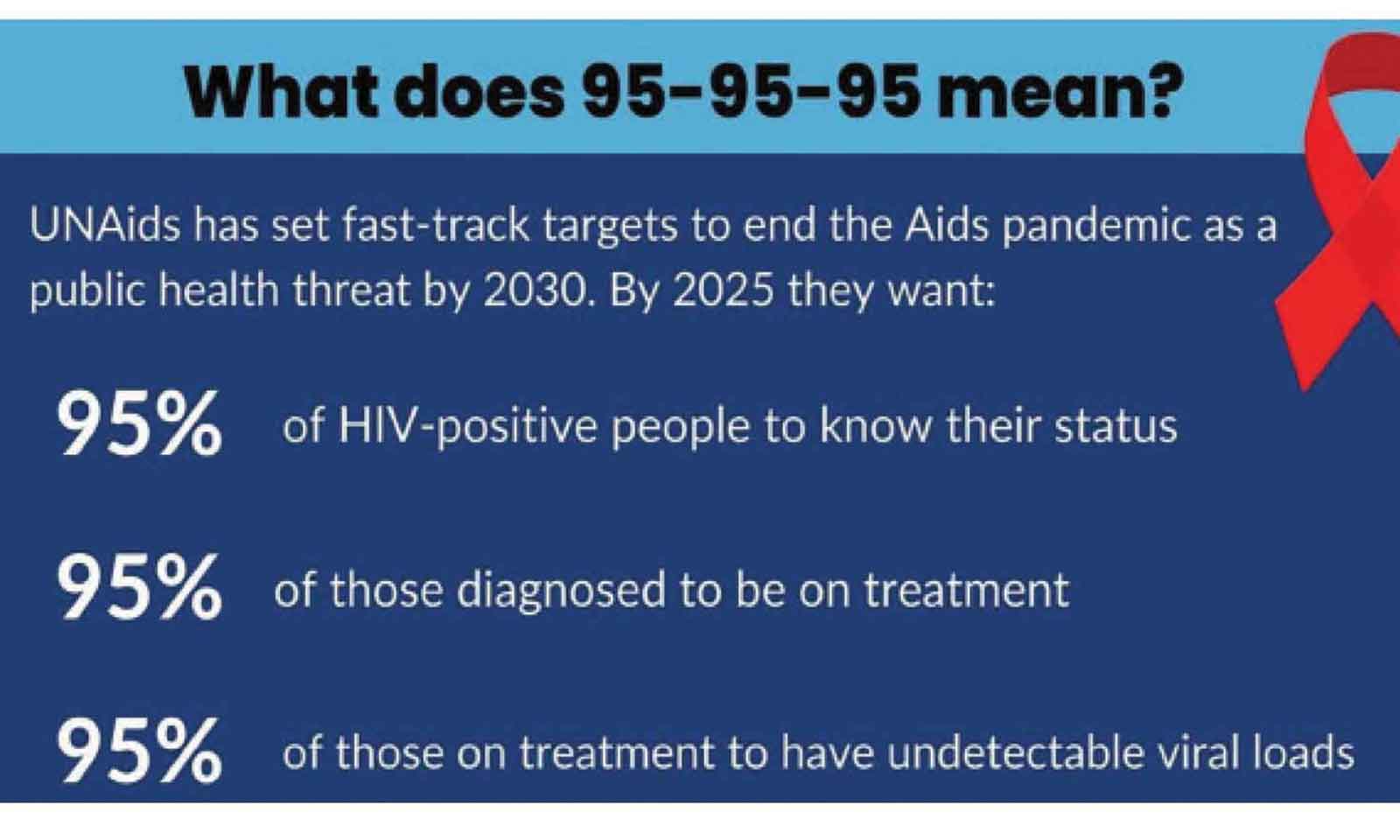
Zimbabwe had already achieved the ambitious 95-95-95 targets, meaning that 95 percent of people living with HIV know their status; 95 percent of those diagnosed were on treatment; and 95 percent of those on treatment have achieved viral suppression.
For health authorities, the year was meant to be a period of strengthening systems, closing remaining gaps and edging closer to the goal of ending AIDS as a public health threat by 2030.
That outlook shifted abruptly in January with the arrival of a new administration in the United States.
This resulted in an immediate halt to funding for programmes supported through USAID and PEPFAR, sending shockwaves across Zimbabwe’s health sector.
National AIDS Council (NAC) chief executive officer Dr Bernard Madzima said the year began on an uncertain note.
“When we entered into 2025, there was a lot of expectation, noting that the country had achieved the 95-95-95 targets. But as early as January, when the new US administration came into office, there was a sudden cut in funding in terms of programmes which were supported by USAID and PEPFAR. That cut in funding resulted in a lot of uncertainty in the sector,” he said.
The implications were far-reaching.
Donor-funded programmes play a critical role in supporting the supply of antiretroviral medicines, laboratory commodities and even the remuneration of health workers.
“It impacted on the supply of ARVs and laboratory commodities. It also impacted on human resources, because those programmes were supporting a lot of health workers in terms of their salaries. What we had anticipated as gradual funding reductions over four or five years suddenly became abrupt,” he said.
With the prospect of treatment disruptions looming, Dr Madzima said NAC, working closely with the Ministry of Health and Child Care, moved swiftly to assess gaps and mobilise domestic resources to stabilise the response.
The speed and effectiveness of that response stands out as the single most significant achievement of 2025.
“We had to quickly assess the situation, identify the gaps and address them using local resources. The most important achievement for 2025 is that we made sure programmes were not disrupted significantly, whether in terms of the health workforce, commodity availability or the services that were being offered,” he added.
By the time the year drew to a close, Zimbabwe had avoided major interruptions to antiretroviral therapy and laboratory services, a feat that health authorities say underscores the value of adaptive planning and domestic resource mobilisation.
“I’m glad to say that we finished 2025 without any major disruption, especially to the supply of ARVs and laboratory commodities,” Dr Madzima said.
“The country had to think outside the box and ensure that we get resources for those commodities.”
Beyond crisis management, 2025 also marked the closing chapter of the Zimbabwe National AIDS Strategic Plan IV (ZNASP IV), which runs from 2020 to 2025.
While a comprehensive end-term evaluation will only be completed in 2026, early signals from routine data and modelling are encouraging.
However, Dr Madzima cautioned that the full picture could only emerge once the cumulative effects of disruptions are properly assessed.
“We still have to measure the impact of Covid-19 from 2020 to 2022, and also the disruptions of this year due to funding. That can only be measured next year, but overall, the data shows that we have done very well,” he said.
Even as national targets show progress, persistent gaps remain, and these are shaping the agenda for the next phase of the response.
Of note is the slower progress among children.
“The 95-95-95 targets mainly speak to the adult age group, but we still lag behind as far as children are concerned. We have not achieved the 95-95-95 in children,” he said.
Mother-to-child transmission of HIV remains a challenge, particularly during pregnancy and breastfeeding, despite years of focused interventions.
Dr Madzima said this would be a priority going into 2026.
Beyond children, HIV incidence remains disproportionately high among certain populations.
While the national incidence stands at around 0.8 percent, some groups face rates nearly double the national average.
“The new infections in the general population are low, but there are sub-populations which are affected more than others. We are talking about sex workers, men who have sex with men, adolescent girls and young women, and unfortunately children through mother-to-child transmission,” Dr Madzima said.
He said urban areas were also showing worrying trends among low- to middle-income groups, underscoring the need for more targeted and context-specific prevention strategies.
It is against this backdrop that Zimbabwe is embracing new biomedical tools that promise to reshape HIV prevention.
Long-acting injectable options are being integrated into the country’s prevention toolkit, complementing existing interventions such as condoms, medical male circumcision, daily oral PrEP and post-exposure prophylaxis.
“The new prevention and treatment methods like long-acting injectables are very important as part of efforts to reduce transmission. They will be integrated into what already exists, they just strengthen what we are already doing,” said Dr Madzima.
Zimbabwe has already begun rolling out the bi-monthly injectable cabotegravir for HIV prevention, targeting individuals at highest risk of infection.
Looking ahead to 2026, the country will pilot Lenacapavir, a twice-a-year injectable prevention option, in partnership with the Global Fund and other partners.
“As we look at the long-acting prevention methods, Cabotegravir and Lenacapavir, we really want to be targeting those key populations to prevent HIV transmission,” Dr Madzima said.
If successful, the Lenacapavir pilot is expected to pave the way for wider national rollout, offering a discreet, longer-lasting option that could significantly reduce new infections among vulnerable groups.
Perhaps the most enduring outcome of 2025, however, lies in the lessons learned.
Dr Madzima said the funding shock reinforced the risks of heavy reliance on external support and sharpened the case for self-reliance.
“The disruption taught us that resources for health programmes should come from within, from Government and domestic resources, because that way we have control,” he said.
The experience has also renewed focus on local manufacturing of health commodities, from medicines to laboratory reagents and equipment, as a way of strengthening national control and resilience.
Looking to the future, Dr Madzima said Zimbabwe was already recalibrating its HIV response.
Work is underway on the Zimbabwe National AIDS Strategic Plan V (ZNASP V), which will guide the response from 2026 to 2030.
The new strategy places sustainability and integration at its core.
“If we are to end AIDS as a public health threat by 2030, HIV programmes can no longer operate as silos,” Dr Madzima said.
ZNASP V is expected to prioritise domestic financing, integrate HIV services into broader health programmes, including non-communicable diseases and epidemic-prone conditions, and align closely with the Government’s universal health coverage and primary health care approach.
As Zimbabwe steps into 2026, the outlook is one of cautious optimism.
The country enters the new year with proof that its HIV response can withstand shocks, a clearer understanding of where gaps persist, and a renewed determination to redesign the response for sustainability.
Dr Madzima said the challenge ahead was not only to sustain progress, but to re-engineer the HIV response for a future defined by self-reliance, integration and precision targeting, ensuring that even in a shifting global landscape, no one is left behind.b

