Rumbidzayi Zinyuke-Health Buzz
Ovarian cancer has long been called a “silent killer” because of the way it creeps into women’s lives with little warning, showing vague symptoms that often mimic harmless conditions.
In Zimbabwe and across the world, this stealth has made it one of the most lethal gynaecological cancers, claiming lives that might otherwise have been saved had the disease been detected earlier or treated more effectively.
According to the World Health Organisation (WHO), more than 313 000 new cases of ovarian cancer were diagnosed worldwide in 2020 and over 207 000 women died from it in the same year.
That makes ovarian cancer the eighth most common cancer among women and one of the top causes of cancer-related deaths.
Although it does not strike with the frequency of breast or cervical cancer, its mortality rate is alarmingly high, primarily because most cases are detected when the disease has already spread beyond the ovaries.
According to the National Cancer Registry report for 2018, ovarian cancer was the sixth most common cancer among women, accounting for 2,4 percent of all cases reported that year.
While the figures may seem small compared with global numbers, they are significant for a country where diagnostic services are limited and cancer reporting systems are still developing.
Experts believe the true burden could be higher, as many cases go undiagnosed or are registered only at very advanced stages. The Zimbabwe National Cancer Registry has consistently highlighted gaps in surveillance.
The risk factors for ovarian cancer are varied, and they reflect the interplay of genetics, biology and lifestyle. Age is perhaps the most striking, with the risk increasing as women grow older, particularly after menopause. Family history also plays a key role; women who inherit certain mutations in genes face a dramatically higher chance of developing ovarian cancer.
This connection has been well documented in Western countries, where genetic testing and counselling are more accessible. In Africa, however, genetic screening remains out of reach for most families, leaving many women unaware of the silent danger that runs in their bloodline.
Beyond age and genetics, reproductive history has also been linked to risk. Women who never have children, who experience late pregnancies, or who have early menstruation and late menopause tend to have a higher likelihood of developing ovarian cancer.
Yet lifestyle factors, increasingly common in modern societies, are emerging as equally important drivers of the disease. Obesity, poor diet, lack of exercise and diabetes all raise the risk. Smoking and alcohol consumption add to the problem, and together, these behaviours are fuelling an increase in ovarian cancer cases among younger women.
The challenge in Africa is that these risk factors are layered onto health systems that struggle to diagnose the disease in time.
Ovarian cancer often announces itself through non-specific symptoms — abdominal bloating, pelvic pain, digestive changes or urinary urgency — that women may dismiss as ordinary discomforts. By the time these signs are recognised as something more serious, the cancer is usually advanced, and treatment options are limited.
Treatment for ovarian cancer globally revolves around a combination of surgery and chemotherapy. When caught early, surgery to remove the ovaries, fallopian tubes, uterus and affected tissues can be curative.
For most women, chemotherapy is prescribed to kill residual cancer cells and prevent recurrence.
Africa, however, faces immense hurdles in applying these treatment standards. Surgical oncology expertise is available but limited, and most advanced procedures are performed only in major cities. Chemotherapy drugs, though central to treatment, are often in short supply in public hospitals. Some patients have to buy their medication privately at costs far beyond their means, leading to treatment delays or incomplete cycles.
Radiotherapy, which sometimes plays a role in palliative care, is also hampered by frequent breakdowns of ageing machines. And while targeted therapies are revolutionising care elsewhere, they remain out of reach for the majority of women.
These resource constraints mean that for many patients, the outcome is determined not only by the biology of the disease but by where they live, how much they earn and how quickly they can access specialist care.
Women in rural areas face the steepest barriers. Travelling to the city for diagnosis and treatment involves high transport costs, time away from family, and often long waiting times in under-resourced facilities. For those who present late, the priority shifts from curing the disease to providing palliative care that manages pain and preserves dignity.
Yet the situation is not without hope. Zimbabwe’s health authorities have included cancer prevention and treatment in the National Health Strategy, and the National Cancer Control Plan outlines steps to strengthen awareness, diagnosis and care. Efforts are underway to decentralise oncology services, strengthen pathology and imaging departments, and improve the supply of essential chemotherapy drugs.
However, prevention and early detection remain critical. While there is no reliable population-based screening test for ovarian cancer comparable to Pap smears for cervical cancer, educating women and health workers to recognise early warning signs can make a difference.
Primary health centres could play a stronger role in referring suspected cases quickly, while investment in diagnostic tests would enable faster confirmation. Public campaigns that promote healthier lifestyles, encouraging exercise, balanced diets, and reduced smoking and alcohol consumption could also help reduce the modifiable risks.
The global burden of ovarian cancer is projected to rise by more than 55 percent by 2050 if no effective interventions are put in place.
For Zimbabwe, where the population of women over 50 is steadily increasing, this means the number of cases could grow significantly in the coming decades. Without investments in health infrastructure, trained personnel and affordable drugs, the country will struggle to keep pace with this rising tide.
What is clear, however, is that ovarian cancer need not remain a silent killer. With stronger awareness, better access to treatment and improved support systems, survival rates can improve.
Women can be empowered with information to take symptoms seriously and seek care early. Families can be educated about the importance of knowing their medical history.
Health systems can also be better equipped to provide the comprehensive care that modern oncology demands.
Ovarian cancer may still carry the weight of silence, but breaking that silence is the first step to saving lives.
For Zimbabwe, the battle is as much about overcoming resource challenges and building robust health systems as it is about treating the disease itself. The statistics tell a sobering story, but they also serve as a call to action.
One that can no longer be ignored if women’s lives are to be protected.
FAST FACTS
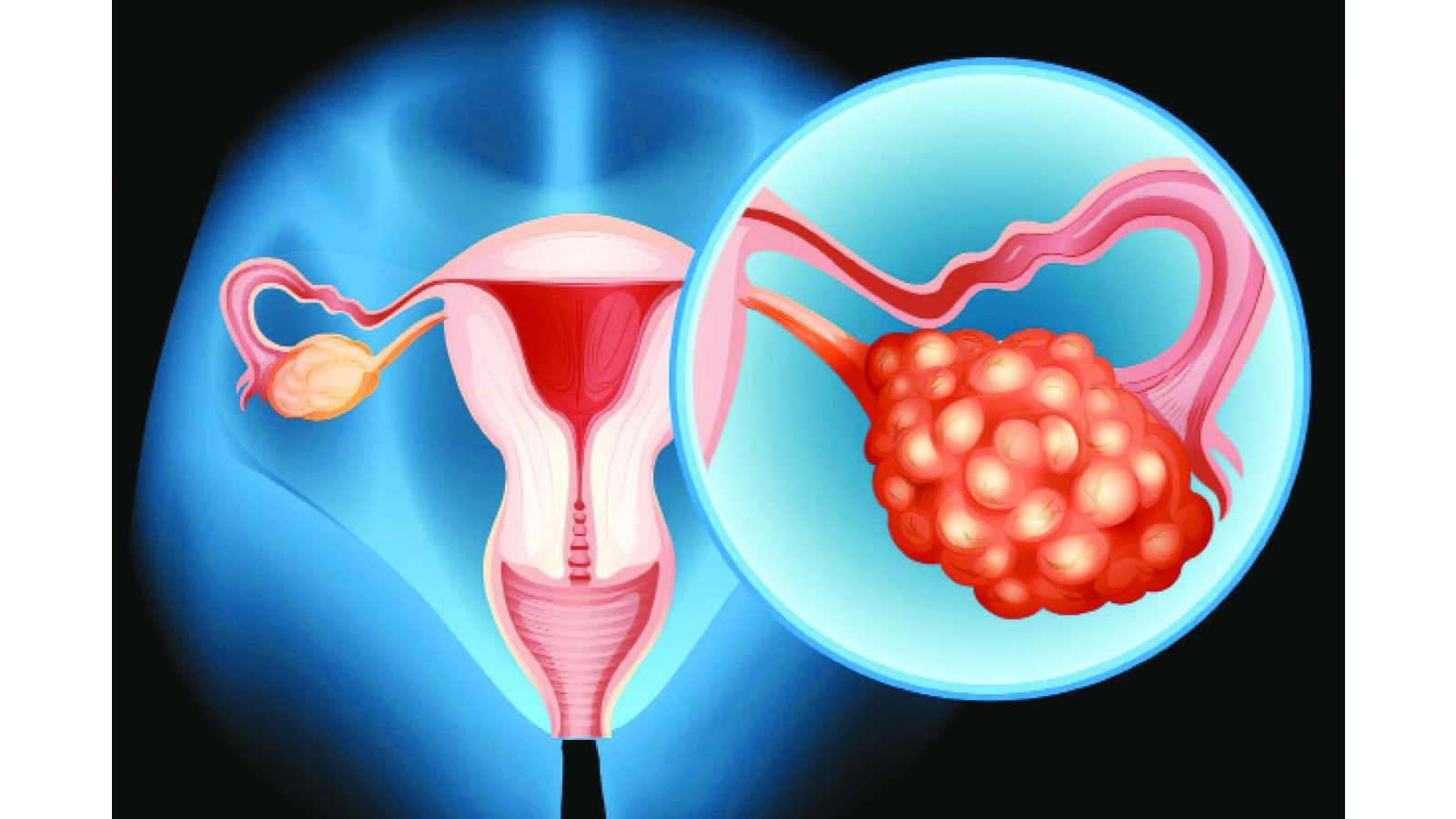
Ovarian cancer occurs when abnormal cells in the ovary, fallopian tube, or peritoneum grow uncontrollably and form a tumor. Most commonly, it is epithelial cancer, starting in the outer cells of the ovary. Symptoms can include bloating, abdominal pain, a feeling of fullness, and urinary changes. Treatment typically involves surgery and chemotherapy, but its effectiveness depends on the cancer’s stage and type.
What is ovarian cancer?
Origin: Ovarian cancer can start in the ovary, but many cases originate in the fallopian tubes or the lining of the abdomen (peritoneum).
Cell types: Ovarian cancers are classified by their cell of origin, with epithelial ovarian cancer being the most common type. Other types include germ cell and stromal tumours.
What causes ovarian cancer?
The exact cause of ovarian cancer isn’t yet known. But some people have a slightly higher risk of developing the condition. Ovarian cancer risk factors include:
Being over the age of 60.
Obesity.
A family history of ovarian cancer (others in your biological family have had the disease) or have inherited a gene mutation (BRCA1 or BRCA2) or Lynch syndrome.
Never being pregnant or having children later in life.
Endometriosis.
There’s also an increased risk of developing ovarian cancer as you grow older.
Hormone therapy with oestrogen after menopause
How does ovarian cancer spread?
If ovarian cancer spreads, it usually does so from your pelvis to your lymph nodes, abdomen, intestines, stomach, chest or liver.
Symptoms
Symptoms can be vague and may be confused with other conditions, especially in the early stages. They can include:
Abdominal bloating or increased size
Pelvic or abdominal pain
Feeling full quickly and loss of appetite
Changes in urination, such as frequent urination or urgency
Changes in bowel habits, like diarrhoea or constipation
Diagnosis and Treatment
Diagnosis: A doctor will likely refer you to a specialist for further tests if ovarian cancer is suspected.
Treatment: Surgery and chemotherapy are the main treatments for ovarian cancer. The specific treatment plan depends on the cancer’s stage, type, and grade.
Prognosis
Early detection is key: The survival rate is higher when ovarian cancer is detected and treated at an earlier, localized stage.
Survival rates: The overall 5-year relative survival rate for ovarian cancer is around 46 percent.
Feedback: [email protected]