
Getrude Chigerwe
Features Correspondent
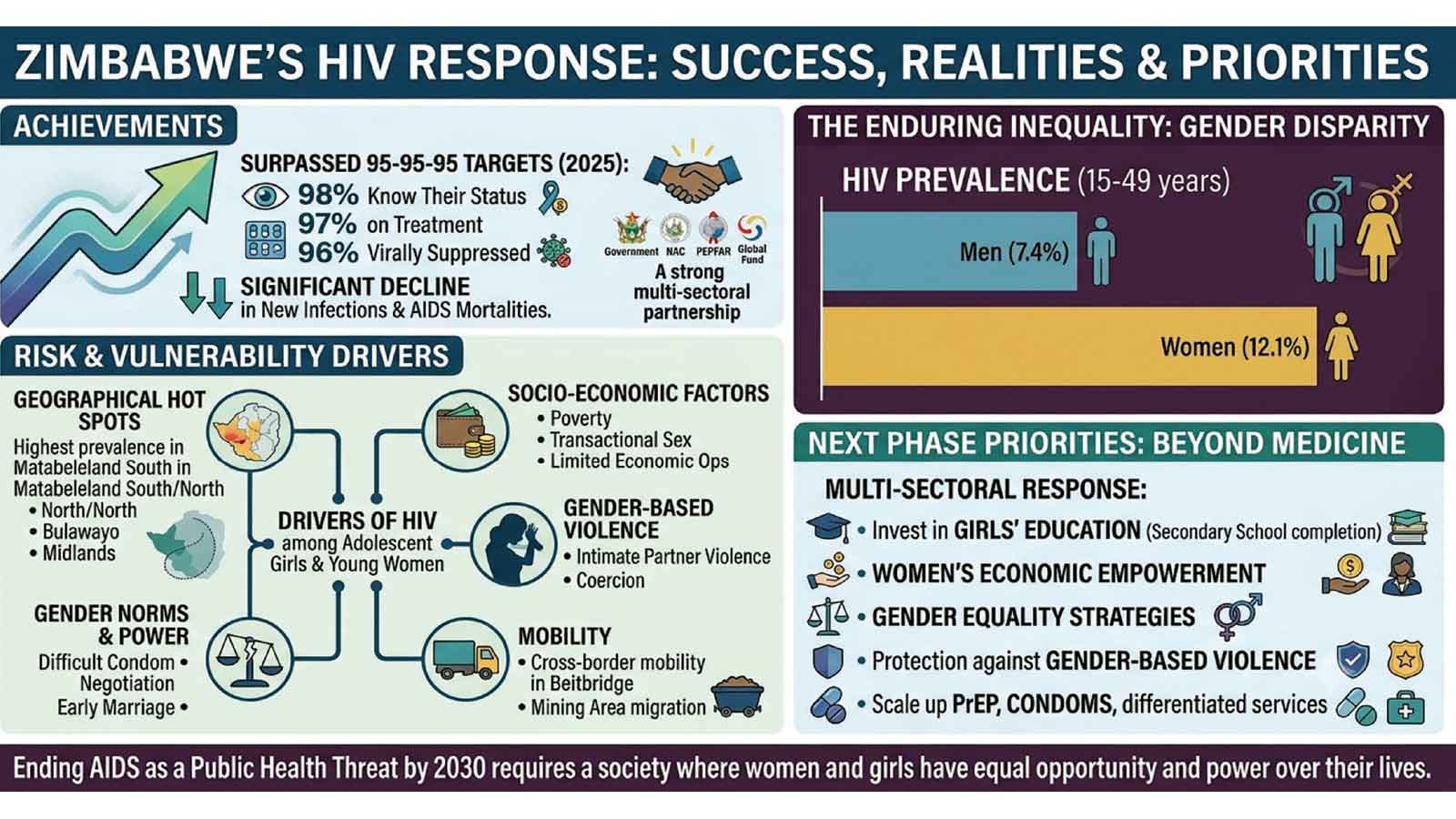
ZIMBABWE’S HIV response is widely regarded as one of the continent’s most remarkable public health success stories, with the country not only meeting, but also exceeding the UNAIDS 95-95-95 targets and significantly reducing new infections.
Yet, the epidemic’s most enduring inequality remains unchanged. Women and girls, particularly adolescents and young women, continue to be infected at far higher rates than men, exposing a challenge that cannot be addressed by medical interventions alone.
An estimated 1,3 million Zimbabweans are HIV positive, placing Zimbabwe among the 10 countries with the highest number of people with HIV.
Although the epidemic has declined significantly since the late 1990s, women remain disproportionately affected.
UNAIDS estimates HIV prevalence among women aged between 15 and 49 at 12,1 percent, compared to 7,4 percent among men, a disparity that reflects deep rooted social and economic inequalities.
Globally, 40,8 million people are HIV positive, and women and girls account for 53 percent of that population.
Southern Africa remains the epicentre of the epidemic, and Zimbabwe continues to carry one of the region’s highest burdens despite its remarkable progress.
Health experts say a complex interplay of biological, social and economic forces shapes women’s heightened vulnerability.
While biology increases susceptibility during unprotected heterosexual intercourse, it explains only part of the gap.
Gender inequality, gender based violence, limited economic opportunities and unequal power dynamics in relationships significantly increase women’s risk.
For many, negotiating condom use remains difficult, especially where financial dependence or fear of violence limits their autonomy.
Survivors of intimate partner violence face even higher risk, making gender based violence both a human rights crisis and a public health concern.
Adolescent girls and young women remain the most vulnerable group. Young women aged between 15 and 24 continue to contract HIV at much higher rates than their male counterparts, often facing early sexual debut, age disparate relationships, poverty driven transactional sex and limited access to youth friendly health services.
A recent study by UN Women and the National AIDS Council highlights this reality, showing that the high HIV incidence among young women in Matabeleland South is rooted in structural and socioeconomic conditions rather than individual behaviours.
The research highlights poverty, cross border mobility, gender based violence, harmful gender norms, school dropout, early marriage and limited access to PrEP as the major forces driving young women’s heightened vulnerability.
Dr Bernard Madzima, chief executive of the National AIDS Council (NAC), has noted that the drivers of HIV among adolescent girls and young women extend beyond the health sector.
“The drivers of HIV among adolescent girls and young women go beyond health. They include poverty, gender inequality, gender-based violence and limited economic opportunities, which is why a multi-sectoral response remains critical”, he said.
The spread of the epidemic varies widely across the country. Matabeleland South records the highest prevalence at 19,4 percent, followed by Bulawayo, Matabeleland North, Masvingo and Midlands. Manicaland has the lowest prevalence at 10,5 percent, though studies suggest it continues to experience relatively high rates of new infections.
Border communities such as Beitbridge face heightened risk due to high mobility among traders, transport operators and migrant workers, creating conditions that increase the likelihood of multiple concurrent partnerships and transactional sex.
Mining areas attract large migrant workforces and commercial sex work, sustaining transmission, while urban centres like Harare and Bulawayo grapple with high population density and social mobility, which increase opportunities for transmission despite better access to services.
In spite of these challenges, Zimbabwe has built one of Africa’s most comprehensive HIV responses.
Through the Ministry of Health and Child Care, the National AIDS Council and partners, including the UN, PEPFAR, the Global Fund and CSOs, the country has expanded access to free HIV testing, counselling and treatment.
More than 1,2 million people are on antiretroviral therapy, and early diagnosis has sharply reduced AIDS related mortalities. Zimbabwe has also excelled in preventing mother to child transmission through routine antenatal testing, immediate treatment initiation and early infant diagnosis.
The country continues to scale up PrEP, voluntary medical male circumcision, condom distribution, viral load monitoring, community based testing and differentiated service delivery models that bring care closer to communities.
These efforts have produced extraordinary results. Zimbabwe is one of the few countries worldwide to achieve and surpass the UNAIDS 95 95 95 targets: 98 percent of HIV positive people know their status, 97 percent of those diagnosed are on treatment, and 96 percent of those on treatment are virally suppressed.
This achievement reflects sustained political commitment, strong partnerships and community driven action.
Yet even with this progress, inequalities persist. Economic hardship continues to push many women and girls into transactional or exploitative relationships.
Stigma still deters some from seeking services, and heavy reliance on donor funding raises concerns about long term sustainability.
On International Women’s Day 2025, UNAIDS executive director Winnie Byanyima captured the heart of the challenge, saying, “There is a deep injustice faced by women and girls, their vulnerability to HIV.
“But when countries work to support girls and enable them to complete secondary school, we keep them safer from HIV, from teenage pregnancy, from violence and child marriage.”
Her words echoed a growing consensus that the next phase of Zimbabwe’s HIV response must confront the structural inequalities that place women and girls at risk.
This means investing in girls’ education, women’s economic empowerment, comprehensive sexuality education, gender equality and stronger protection against gender based violence.
Zimbabwe has shown that determined leadership, strong partnerships and community engagement can reverse even the most severe epidemics. But the country’s progress must benefit everyone equally.
Ending AIDS as a public health threat by 2030 will require more than medicine. It will require a society where women and girls have equal access to education, healthcare, economic opportunity and the power to make decisions about their own lives.

