Rumbidzayi Zinyuke
Health Buzz
Before hospitals, scans, medicines and specialist consultations, there is often a family trying to do its best.
It could be a daughter helping her ageing mother eat after a stroke, a husband sitting beside his wife through another painful night of cancer, or grandparents caring for a relative living with advanced HIV.
They are not doctors or nurses, yet they become caregivers overnight, learning through trial and error while juggling emotional, physical and financial burdens.
For many Zimbabwean families, this journey is made even more difficult by a health system that can be complex to navigate.
Appointments at different hospitals, referrals between specialists, the rising cost of treatment and uncertainty over what lies ahead often leave patients and their loved ones overwhelmed.
This is where palliative care becomes not just an option but an essential part of healthcare.
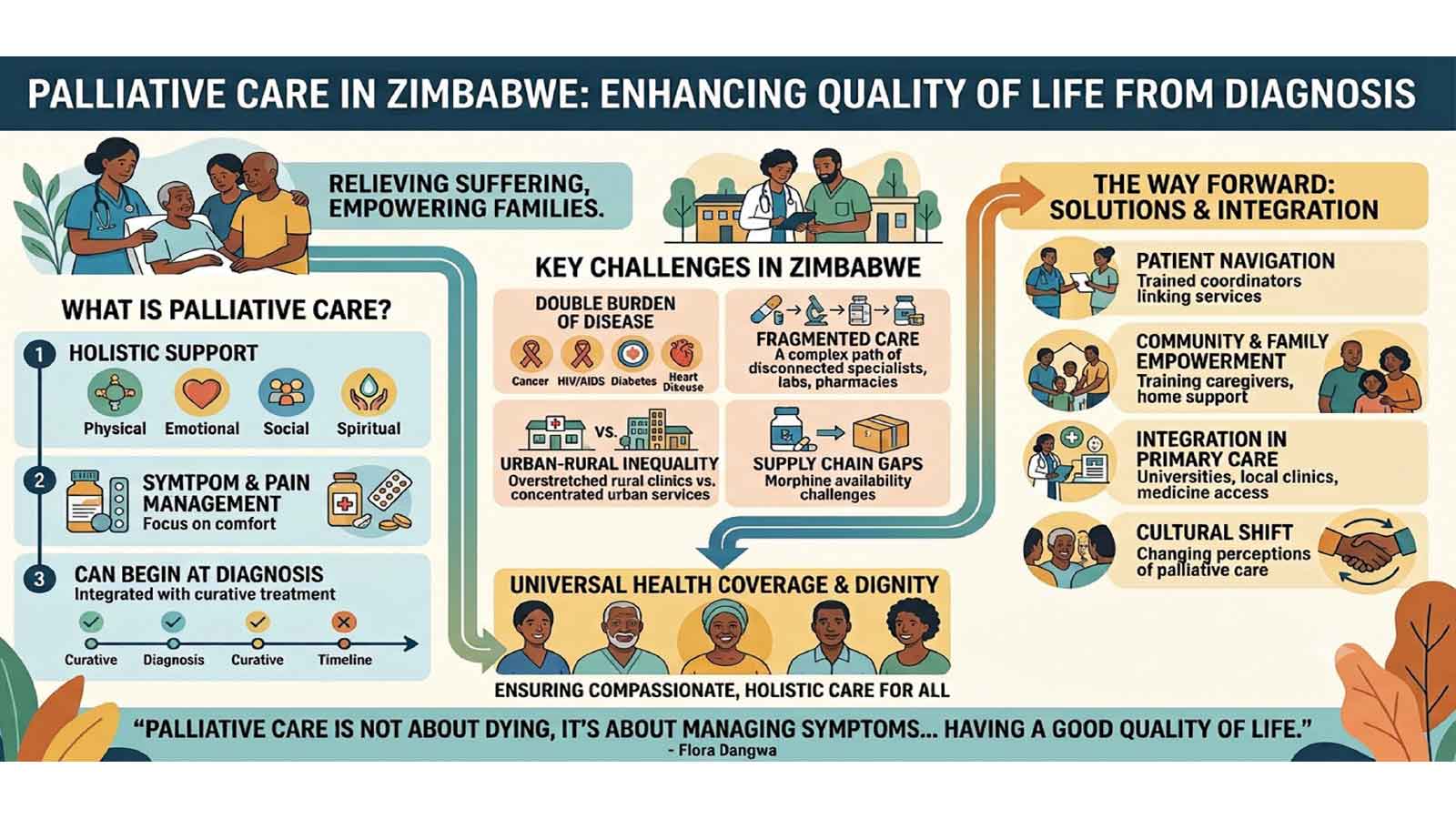
Contrary to the common misconception that palliative care is only for people who are about to die, it is about helping people with serious illnesses live as comfortably and as fully as possible.
It focuses on relieving pain and other distressing symptoms while providing psychological, emotional, social and spiritual support to both patients and their families.
More importantly, it can begin at the time of diagnosis and continue alongside curative treatment.
As Zimbabwe grapples with an increasing burden of cancer, heart disease, diabetes and other chronic illnesses, alongside HIV and tuberculosis, experts say the country can no longer afford to view palliative care as a service reserved for the final days of life.
Globally, the need for palliative care is growing at an unprecedented rate.
According to the World Health Organisation (WHO), more than 56 million people require palliative care each year, yet only about 14 percent receive it. Nearly 80 percent of those in need live in low- and middle-income countries, where health systems often struggle with limited resources.
Zimbabwe mirrors this global challenge.
Despite being one of the first African countries to establish organised palliative care services through Island Hospice decades ago, access remains limited.
Experts estimate that only about 10 percent of Zimbabweans who need palliative care are able to receive it.
This means thousands of patients continue to experience unnecessary pain and suffering, while families shoulder enormous responsibilities with little support.
Ironically, Zimbabwe was once regarded as a continental leader in palliative care.
The country developed one of Africa’s earliest hospice models and later adopted the National Palliative Care Policy in 2014, followed by the inclusion of palliative care in the National Health Strategy.
These milestones demonstrated recognition that caring for people with life-limiting illnesses should form part of an effective healthcare system.
However, while policy development has progressed, implementation has not always kept pace.
Countries such as Uganda have since overtaken Zimbabwe by integrating palliative care into universities, primary healthcare services and medicine supply systems, ensuring that patients can access support much earlier in the course of illness.
One of the biggest challenges highlighted by experts at a recent meeting held in Harare is that healthcare often remains fragmented.
A patient diagnosed with cancer, for example, may have to move between surgeons, oncologists, radiotherapists, laboratories, pharmacies and community services. Each professional may provide excellent care individually, yet patients are frequently left to coordinate appointments, organise transport, communicate between health providers and make complex medical decisions while battling serious illness.
Families, already coping with fear and uncertainty, often become managers of an intricate healthcare system they barely understand.
The consequences are delayed treatment, poor symptom control, repeated hospital admissions and unnecessary emotional distress.
This has prompted growing calls for patient-centred models of care that improve communication and coordination between healthcare providers.
Palliative care specialists believe one practical solution lies in patient navigation, where trained professionals help patients and families understand treatment options, coordinate services and access psychosocial support throughout their illness.
Such an approach is particularly important as Zimbabwe experiences what experts describe as a “double burden” of disease.
While infectious diseases such as HIV and tuberculosis remain significant public health concerns, non-communicable diseases are rising rapidly.
Cancer cases continue to increase, cardiovascular diseases are becoming more common, diabetes is affecting more families, and Zimbabwe’s population is gradually ageing. People are living longer, but many are living with multiple chronic conditions requiring continuous support rather than isolated episodes of treatment.
This changing disease pattern means healthcare can no longer focus solely on curing disease. It must also prioritise quality of life.
Palliative care, therefore, becomes an important component of Universal Health Coverage by ensuring that people receive compassionate, holistic care regardless of whether their illness can be cured.
As palliative care specialist Dr Dickson Chifamba noted, “Palliative care is an essential component of Universal Health Coverage, specifically for the Sustainable Development Goal three, which talks about access to health.”
His observation reflects growing international recognition that pain relief, dignity and emotional support should be available to everyone living with serious illness, not only those who can afford specialised private care.
Yet access remains highly unequal.
Most palliative care services are concentrated in Zimbabwe’s urban centres, leaving rural communities with few options beyond overstretched clinics.
Ironically, almost 68 percent of Zimbabwe’s population lives in rural areas.
Distance, transport costs and shortages of specialised healthcare workers make it difficult for many patients to receive regular care, forcing families to manage complex illnesses at home.
This is where communities themselves become indispensable.
Studies show that almost 95 percent of care provided to people nearing the end of life comes not from hospitals but from families, neighbours and communities.
Zimbabwe’s culture of collective responsibility has long enabled relatives and neighbours to support one another during illness. Experts believe this social capital should become one of the country’s greatest strengths in expanding palliative care.
Rather than relying exclusively on hospitals, they say communities can be empowered through caregiver training, better referral systems and stronger links with healthcare professionals.
Simple interventions such as teaching family members how to manage pain, recognise warning signs or provide basic nursing care can dramatically improve patients’ quality of life while reducing unnecessary hospital admissions.
Equally important is changing public perceptions.
Many people still associate palliative care with giving up hope or preparing for death.
This misunderstanding often delays referrals until patients are in the final stages of illness, depriving them of months or even years of symptom relief and emotional support.
Researcher and palliative care nurse Flora Dangwa challenged this misconception.
“Palliative care is not about dying, it’s about managing symptoms, getting coordinated care, people having a good quality of life and having a good quality of death,” she said.
Her words capture the true purpose of palliative care, enabling patients to live as well as possible for as long as possible.
Another obstacle is limited awareness among healthcare professionals themselves.
Although Zimbabwe has made progress by introducing postgraduate palliative care training at several universities and incorporating elements of palliative care into oncology nursing programmes, specialist training remains limited.
Referral pathways are often unclear, resulting in many eligible patients never being referred for specialist support.
Pain management also remains a persistent concern.
According to Dr Chifamba, access to essential medicines, including morphine for severe pain, continues to be affected by supply chain challenges, leaving some patients to endure unnecessary suffering despite affordable solutions already being implemented successfully in countries such as Uganda.
Experts argue that improving medicine availability, strengthening primary healthcare, investing in workforce development and integrating palliative care into routine services would significantly improve patient outcomes.
Ultimately, conversations about palliative care are conversations about dignity.
They are about ensuring that no Zimbabwean faces serious illness alone, that families are supported rather than overwhelmed, and that healthcare extends beyond curing disease to caring for people.
As the country works towards Universal Health Coverage, expanding access to palliative care should no longer be viewed as an optional extra, but as a fundamental measure of a compassionate and equitable health system.
After all, while medicine cannot always add years to life, good palliative care can add life to those years, making every moment count for patients and the families who walk beside them.
Feedback: [email protected]