

Robin Muchetu, Senior Reporter
A passive and unresponsive child who failed to thrive much as other newly borns would do led one attentive mother from Triangle in Chiredzi District to seek medical attention.
The mother, Ms Lorriane Mwale* noticed that her child was not behaving the way other babies normally do and it triggered the need to find answers to her baby’s condition.
“I gave birth to a healthy baby girl in 2006 and when she was around three months, people would tell me that my baby is very quiet as she never used to cry, if she wanted a nappy change she would just whimper very softly and was not as active as other babies,” said Ms Mwale.
As weeks progressed, the “quiet and peaceful” baby Nomsa* suddenly stopped breastfeeding but never raised an alarm immediately as the mother had started supplementing with other foods.
“At six months she stopped feeding and could not suckle anymore, I tried baby formulas and she wouldn’t tolerate them. I then moved to feeding her with mashed bananas and butternuts that she would eat. She, however, failed to eat baby cereals. I then discovered that she could not take any lactose in her system,” she said.
Ms Mwale then noticed a change in the skin colour in her daughter.
“I was in the dark and never understood why my child was not feeding and why she was not as playful as other kids. I noticed when she was a year old, there were patches on her skin that were much lighter than the rest of her body and she had watery eyes.
“Again, she was not as big as my first child in terms of weight and chubbiness. It wasn’t until she turned two and a half years old that she had a chronic fit and she just froze, which scared me. I then sought medical attention where I was told that she had sickle cell anaemia. So, she had various blood tests, and began to have intense epilepsy,” she said.
Following the first episode of seizures, she started having more seizures that presented with terrifying jerks. The severe seizures were accompanied by a swollen stomach and she could not pass urine or stool and Ms Mwale would spend days on end in hospital with her daughter.
“That became the story of my life for the following two years as my daughter was in and out of hospital. Eventually at four years old, I took her for several scans and discovered that she also had a gall stone.
The doctors then put everything together trying to assess the root cause of her several ailments, they did more blood tests and again, they confirmed that she had the sickle cell anaemia,” she said.
Nomsa is one of the approximately 1 000 children born with sickle cell disease every day in Africa, making it the most prevalent genetically-acquired disease in the region.
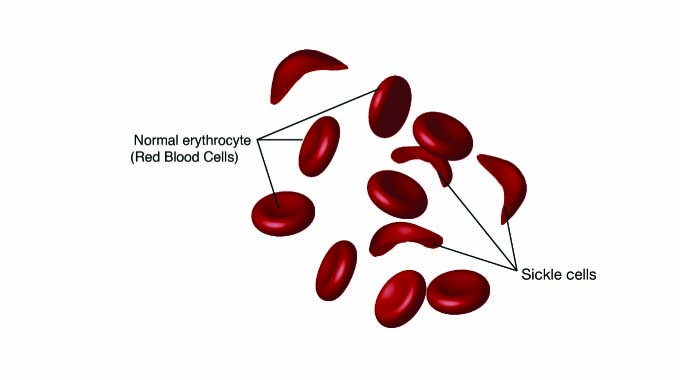
More than half of these children die before they reach the age of five, usually from infection or severe anaemia. Sickle cell disease is an inherited blood disorder that shortens red blood cell survival, causing anaemia—often called sickle cell anaemia.
Poor blood oxygen levels and blood vessel blockages in people with sickle cell disease can cause extreme pain in the back, chest, hands and feet as well as severe bacterial infections.
During the recent 72nd African Regional Committee for Africa, African Health Ministers launched a campaign to ramp up awareness, bolster prevention and care to curb the toll of sickle cell disease, one of the most common illnesses in the region but which receives inadequate attention.
Zimbabwean Minister of Health and Child Care General (Rtd) Dr Constantino Chiwenga attended the engagement where it was highlighted by the World Health Organisation (WHO) that an estimated more than 66 percent of the 120 million people affected worldwide by sickle cell disease live in Africa. Dr Matshidiso Moeti, WHO Regional Director for Africa highlighted that most African countries lacked resources to provide care for people with sickle cell disease.

“Most African countries do not have the necessary resources to provide comprehensive care for people with sickle cell disease despite the availability of proven cost-effective interventions for prevention, early diagnosis and management of this condition.
We need to shine the spotlight on this disease and help improve the quality of life of those living with it,” she said.
WHO highlighted that due to the absence of newborn screening programmes and surveillance across the region, there is a lack of accurate and reliable data on the disease.
Additionally, they say data collection for sickle cell disease is not included in most national population-wide surveys and these data gaps have negatively impacted the prioritization and allocation of resources for the disease.
“We can no longer ignore the significant burden caused by sickle cell disease. We must do more to improve access to treatment and care, including counselling and newborn screening by ensuring that programmes are decentralized and integrated with services being delivered to communities and at primary health care level,” added Dr Moeti.
Ms Mwale said although her daughter, now 16, managed to get some medical help, it was taxing both financially and emotionally.
“For me it was having faith in the medical system in Zimbabwe and walking with God. I was fortunate enough to be working for a private company that had a private hospital and I had access to peadiatricians, neurosurgeons, and a whole range of specialist doctor care. We diligently followed all the prescribed medication for her various conditions including epilepsy,” she said.
She added that her daughter stopped having seizures when she was eight years old.
“Though I am not too sure if the sickle cell anaemia has disappeared, she occasionally has loads of gastric reflux but it is not as bad as it was before. At least now she can go for at least three to six months without having this problem.”
Ms Mwale said it was very important for parents and guardians to be attentive to their children as they grow because they run the risk of leaving their children to suffer when they have medical conditions that the child cannot explain.
Dr Moeti stressed the need for greater investment and stronger collaboration and partnerships to help stem the tide of rising cases of sickle cell disease in Africa.
WHO noted that beyond its public health impact, sickle cell disease also poses numerous economic and social costs for those affected and their families and can interfere with many aspects of patients’ lives, including education, employment, mental and social well-being and development.

